[New post] Cerebral Edema and Diabetic Ketoacidosis: Rebaked
Kendra Jackson posted: " Authors: Drs. Kendra Jackson and Rebecca Raffler While we've gotten to snack on a Morsel on this subject before, new guidelines and research surrounding DKA and cerebral edema have come to light since the first go 'round! Thankfully, Dr. Fox wasn" Pediatric EM Morsels
While we've gotten to snack on a Morsel on this subject before, new guidelines and research surrounding DKA and cerebral edema have come to light since the first go 'round! Thankfully, Dr. Fox wasn't too "salty" when we asked to rehydrate this topic. Rates of type 1 diabetes have increased since theCOVID-19 pandemic. As a result, the rates of DKA andHyperglycemic Hyperosmotic Syndromeare on the rise. Cerebral edema is the most feared emergent complication of pediatric diabetic ketoacidosis. Children with moderate to severe DKA admissions have been shown to drop IQ points and it is theorized that cerebral edema is the culprit. To help us avoid this, let's take a minute to review the current recommendations for Cerebral Edema and Diabetic Ketoacidosis.
Pediatric Diabetic KetoAcidosis: Basics
To consider the diagnosis of diabetic ketoacidosis, there must be three major criteria:
Hyperglycemia
Ketone formation
Metabolic acidosis
Hyperglycemia
Ketosis
Acidosis
Relatively Higher Glucose to Baseline
Can be measured in Urine or Serum
Bicarb < 18 mmol/L
Persistent
Beta-Hydroxybutyrate level >/= 3 mg/dL
pH < 7.3
Glucose > 200 mg/dL
Moderate or Large Ketonuria
The severity of DKA is categorized by the degree of acidosis
Mild: venous pH < 7.3 or serum bicarbonate between 11-17 mmol/L
Moderate: venous pH < 7.2 or serum bicarbonate between 5-10 mmol/L
Severe: venous pH < 7.1 or serum bicarbonate <5 mmol/L
Treatment for DKA is centered around the following principles
Fluid resuscitate and rehydrate
Insulin, IV or subq, to counteract ketosis/acidosis
Giving glucose PRN to promote anabolism and avoid hypoglycemia (due to insulin therapy)
Correcting hypokalemia
After initial fluid resuscitation with crystalloids, we need to provide insulin as safely and conveniently as possible.
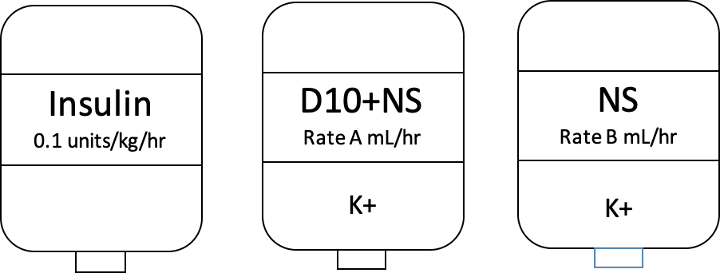
The triple bag system was developed to easily adjust the glucose infusion rate as needed to avoid hypoglycemia and hypokalemia.
Here are our three bags. Some intuitions refer to this system as the "Two-bag" system, but why leave out the most important bag? Insulin!
We have a cheat sheet at our institution to provide weight-based titration protocols for our nursing colleagues. Take a peak...
Cerebral Edema and Diabetic Ketoacidosis
Neuroimaging studies have shown that Cerebral Edema is not rare.
Mental status abnormalities (GCS scores <14) occur in approximately 4%–15% of children treated for DKA and are often associated with mild cerebral edema on neuroimaging.
The mortality rate for cerebral edema is 21%–24%.
Lesson = treat early!
The exact mechanism is not known…
It was previously believed that it was due to rapid changes in serum osmolality during initial fluid resuscitation.
However, new information tells us that the hyperinflammatory state in DKA with cerebral hypoperfusion may play a big role.
Clinically significant injury generally presents within the first 12 hours of treatment, but as long as 24-48 hours out
The diagnosis is clinical! Neuroimaging is NOT required.
Debunked Risk Factors for Developing Cerebral Edema
Generally, there is an absence of evidence that associates higher initial glucose levels, higher osmolality, or declines in these values during treatment and our risk for developing cerebral edema.
One study found no difference in frequency of mental status change and cerebral injury in kids who had a decline in sodium vs. kids who did not.
Cerebral edema CAN present prior toinitiation of treatment for DKA, including in some children with diabetes who died at home.
Risk Factors that seem to stay consistent:
Administration of Bicarb for correction of acidosis has been shown to be associated with cerebral edema and DOES persist after correcting for severity of DKA!
Kids < 5 years of age
New onset of diabetes at presentation
Longer duration of symptoms
Severity of acidosis
Elevated BUN
Greater degree of dehydration and hyperventilation
Cerebral Edema and DKA: Diagnostic Considerations
Early detection and treatment is the best means to prevent brain injury and death.
Headaches can be common at initial presentation and are generally acceptable.
They should provoke our increased vigilance - pay closer attention if they worsen after starting therapy.
Altered mentation, confusion, fluctuating level of consciousness
Heart rate decelerations (decline of more than 20 bpm) not due to improved hydration or sleep
Age-inappropriate incontinence
Minor Criteria
Vomiting
Headache
Lethargy or being not easily aroused from sleep
Diastolic BP > 90 mmHg
Age < 5 yrs
Having either 1 Diagnostic Criterion, 2 Major Criteria, or 1 Major and 2 Minor criteria lead to 92% sensitivity and 96% specificity for recognition of Cerebral Edema early enough for intervention.
A critical MORSEL is that every child you treat for DKA needs to have an initial thorough neuro exam including cranial nerves and then frequent neuro reassessments… and document it (so your colleagues who take over care for the kid can know if there has been a change)!
Alternately, Mannitol 1 g/kg over 20 minutes, but it is associated with worsening diaresis
Repeat dose after 30 minutes if no improvement
Head of Bed at 30 degrees
Consider Intubation
Reserve only for those with respiratory failure secondary to severe neurologic compromise
AVOID giving bicarb… as stated above, this is associated with worse outcomes
Moral of the Morsel
DKA - An actually USEFUL Abreviation! Is your patient hyperglycemic, acidotic, with ketonuria? Then we've likely got DKA.
Triple bag, triple bag, triple bag! Insulin (in Bag #1) is for the Acidosis. Prevent the hypoglycemia is adding Glucose and use the other two bags to make timely adjustments of glucose infusion rate.
You don't need a CT or MRI for that! Cerebral edema is a clinical diagnosis – do NOT delay treatment of cerebral edema for imaging!
Get Salty! If you are concerned for developing cerebral edema, consider using Hypertonic Saline over Mannitol.
Weiss A, Donnachie E, Beyerlein A, Ziegler A, Bonifacio E. Type 1 Diabetes Incidence and Risk in Children With a Diagnosis of COVID-19. JAMA. 2023;329(23):2089–2091. doi:10.1001/jama.2023.8674
Chase H, Garg S, Jelley D. Diabetic ketoacidosis in children and the role of outpatient management. Pediatr Rev. 1990;11:297-304
von Oettingen J, Wolfsdorf J, Feldman HA, Rhodes ET. Use of serum bicarbonate to substitute for venous pH in new-onset diabetes. Pediatrics. 2015;136(2):e371-e377.
Dunger D, Sperling M, Acerini C, et al. ESPE / LWPES consensus statement on diabetic ketoacidosis in children and adolescents. Arch Dis Child. 2003;89:188-194
Chapter 11: Diabetic Ketoacidosis and Hyperglycemic Hyperosmolar State. Nicole Glaser, Maria Fritsch, Leena Priyambada, Arleta Rewers, Valentino Cherubini, Sylvia Estrada, Joseph I. Wolfsdorf, Ethel Codner
Glaser, N, Fritsch, M, Priyambada, L, et al. ISPAD Clinical Practice Consensus Guidelines 2022: Diabetic ketoacidosis and hyperglycemic hyperosmolar state. Pediatr Diabetes. 2022; 23( 7): 835- 856. doi:10.1111/pedi.13406








No comments:
Post a Comment